Article Type: Case Report
Bilateral acute blindness revealing a postoperative PRES syndrome after nephrectomy: A case report
Manal Ibrahimi1; Mohammed Mrabti2*; Mohammed Tetou2; Younes Boukhlifi2; Abdessamad El Bahri2; Mohammed Alami2; Ahmed Ameur2
1Department of Radiology, Mohammed V Military Hospital, Mohammed V University, Rabat, Morocco.
2Department of Urology, Mohammed V Military Hospital, Mohammed V University, Rabat, Morocco.
*Corresponding author: Mohammed Mrabt
Department of Urology, Mohammed V Military Teaching Hospital, Faculty of Medicine and Pharmacy, Mohammed V University in
Rabat, Rabat, Morocco.
Email ID: dr.mohammedmrabti@gmail.com
Received: Sep 17, 2025
Accepted: Sep 22, 2025
Published Online: Sep 29, 2025
Journal: Annals of Medical Case Reports and Reviews
Copyright: © Mrabti M et al. (2024). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Ibrahimi M, Mrabti M, Tetou M, Boukhlifi Y, Bahri AE, et al. Bilateral acute blindness revealing a postoperative PRES syndrome after nephrectomy: A case report. Ann of Med Cas Rep & Reviews. 2025; 1(1): 1007.
Introduction
Posterior Reversible Encephalopathy Syndrome (PRES) is a rare neurological condition, both clinical and radiological, characterized by reversible brain abnormalities, primarily vasogenic edema involving the posterior regions of the brain. It typically presents with headaches, visual disturbances, seizures, and altered mental status. First described by Hinchey et al. in 1996 [1], it occurs in diverse contexts such as acute hypertension, renal failure, immunosuppressive therapy, and certain postoperative situations.
The underlying pathophysiology of PRES is related to impaired cerebral autoregulation and disruption of the blood– brain barrier, leading to vasogenic edema [2]. While extensively documented in obstetric and oncological settings, its occurrence in non-neurological, especially urological, surgery remains exceptional.
We report here the case of transient acute bilateral blindness in a patient who underwent nephrectomy for complicated xanthogranulomatous pyelonephritis, with postoperative brain MRI confirming PRES.
Case report
A 54-year-old woman (H.B.) with a 12-year history of insulin dependent diabetes was followed for longstanding right renal lithiasis disease, recently complicated by pyonephrosis. Her condition worsened with recurrent fever and impaired general health. Abdominal imaging revealed parenchymal destruction of the right kidney consistent with xanthogranulomatous pyelonephritis.
Given the irreversible renal damage and lack of response to medical therapy, a right nephrectomy via lombotomy was performed. The surgery was uneventful. The patient received two units of packed red blood cells intraoperatively, followed by another unit postoperatively for moderate anemia correction.
On postoperative day 2, she suddenly developed acute bilateral blindness without other neurological symptoms. Blood pressure was moderately elevated (150/95 mmHg).
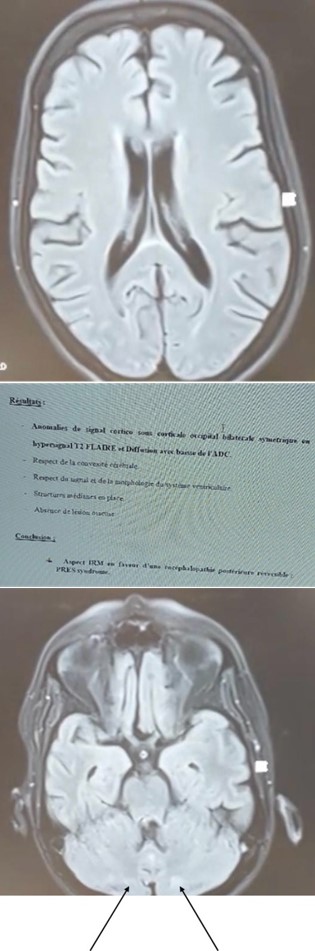
Emergency brain CT revealed no abnormalities. Ophthalmological examination, including funduscopy and visual fields, was unremarkable. Same-day brain MRI showed bilateral occipital FLAIR hyperintensities without diffusion restriction, typical of PRES (Figure 1).
Management was conservative, with strict glycemic and blood pressure control. The course was favorable, with progressive visual recovery starting on day 4 and complete resolution by day 6 (ad integrum).
Discussion
Our case represents the first report in the literature of PRES syndrome occurring after urological surgery.
PRES is increasingly recognized through brain MRI, yet often overlooked in postoperative contexts outside neurology and obstetrics [1]. This observation illustrates an atypical but documented form of PRES, presenting after complex urological surgery with acute isolated cortical blindness.
Two main pathophysiological mechanisms have been proposed [2]:
1. Cerebral hyperperfusion due to autoregulatory dysfunction, commonly triggered by acute hypertension.
2. Endothelial dysfunction, favored by metabolic diseases (diabetes, renal failure), infections, or transfusions.
In this case, multiple contributing factors were identified: long-standing diabetes, chronic renal impairment from prolonged renal destruction, multiple blood transfusions [3,4], and postoperative systemic inflammation promoting cytokine release.
Bilateral cortical blindness is a rare presentation of PRES, reported in about 40% of cases [5,6]. Only MRI allows a definitive diagnosis, showing occipital FLAIR hyperintensities.
Similar cases have been reported following orthopedic surgery [7], cesarean section [8], tumor resection [9], and massive transfusions [3]. All highlight the importance of early diagnosis and conservative management.
To our knowledge, this is the first reported case of PRES following urological surgery for xanthogranulomatous pyelonephritis. Early recognition and multidisciplinary management are essential to avoid misdiagnosis.
Recent literature also implicates surgical stress-induced systemic inflammation, with cytokine release (TNF-α, IL-6) altering blood–brain barrier permeability, potentially leading to PRES even without severe hypertension [10]. Transfusion-related immune and vascular effects must also be considered, as PRES has been documented after massive transfusions in postoperative hemorrhagic contexts [11].
The preferential occipital involvement remains unexplained but may relate to reduced sympathetic innervation of posterior cerebral arteries, rendering them more vulnerable to hyperperfusion and endothelial dysfunction [12].
Differential diagnoses include ischemic stroke, metabolic encephalopathy, focal seizures, optic neuritis, and cortical degenerative disorders. However, the rapid recovery and typical MRI features support PRES. The swift visual recovery in this case reinforces its reversible nature when diagnosed early [13].
Conclusion
PRES should be suspected in the postoperative setting in any case of acute unexplained bilateral blindness, particularly in high-risk patients (diabetes, renal failure, transfusions). This case emphasizes the crucial role of early MRI-based diagnosis and tailored conservative management, ensuring excellent prognosis.
References
- Frati A, et al. Can post-operative PRES be considered an insidious rare surgical complication? Brain Sci. 2023; 13: 706.
- Gurumukhani JK, Patel HD. Posterior reversible encephalopathy syndrome following blood transfusion: a rare case report. Open Neurol J. 2021; 15: 31–5.
- Mohanty G, Sridivya C. PRES: a rare and reversible cause of vision loss. IJAR. 2020.
- Dugar D, et al. Postoperative idiopathic PRES. J Case Rep. 2021.
- Ismail FS, et al. A broad spectrum of PRES: a case series. BMC Neurol. 2021; 21: 408.
- Shah HH, et al. PRES following postpartum eclampsia. Clin Case Rep. 2024.
- Kueper J, et al. PRES after spinal deformity surgery. Am J Orthop. 2015.
- Mudgal SK, et al. Atypical PRES presentation. Int J Med Res. 2019.
- Calderon C, et al. PRES after ependymoma resection. Int J Surg Case Rep. 2024.
- Fischer M, Schmutzhard E. Posterior reversible encephalopathy syndrome. J Neurol. 2017; 264: 1608–16.
- Rao M, et al. PRES in the postoperative setting: role of transfusion and systemic inflammation. Neurol India. 2022; 70: 145–8.
- Bartynski WS. Posterior reversible encephalopathy syndrome, part 1: fundamental imaging and clinical features. AJNR Am J Neuroradiol. 2008; 29: 1036–42.
- Liman TG, Siebert E, Endres M. Posterior reversible encephalopathy syndrome. Curr Opin Neurol. 2019; 32: 25–35.